Hair loss in women
requires a
different approach.
Many women experience visible hair thinning — yet most hair clinics are built around men. At Pure Line, our core team treats female hair loss with the medical evaluation, careful planning, and softer aesthetic approach it deserves.

Female hair loss requires
a fundamentally different approach.
The anatomy, the patterns, the causes, and the solutions — female hair loss is not a smaller version of male hair loss. It demands its own science, its own artistry, and its own standards of care.
Diffuse Thinning Pattern
Women rarely lose hair in defined patches. Instead, thinning tends to be diffuse — affecting density across the entire crown while the hairline remains largely intact. This creates unique surgical planning challenges.
Medical Complexity First
Female hair loss frequently has hormonal, nutritional, or dermatologic roots — thyroid imbalance, iron deficiency, postpartum shedding. These must be investigated and stabilised before surgery is appropriate.
Hairline as Identity
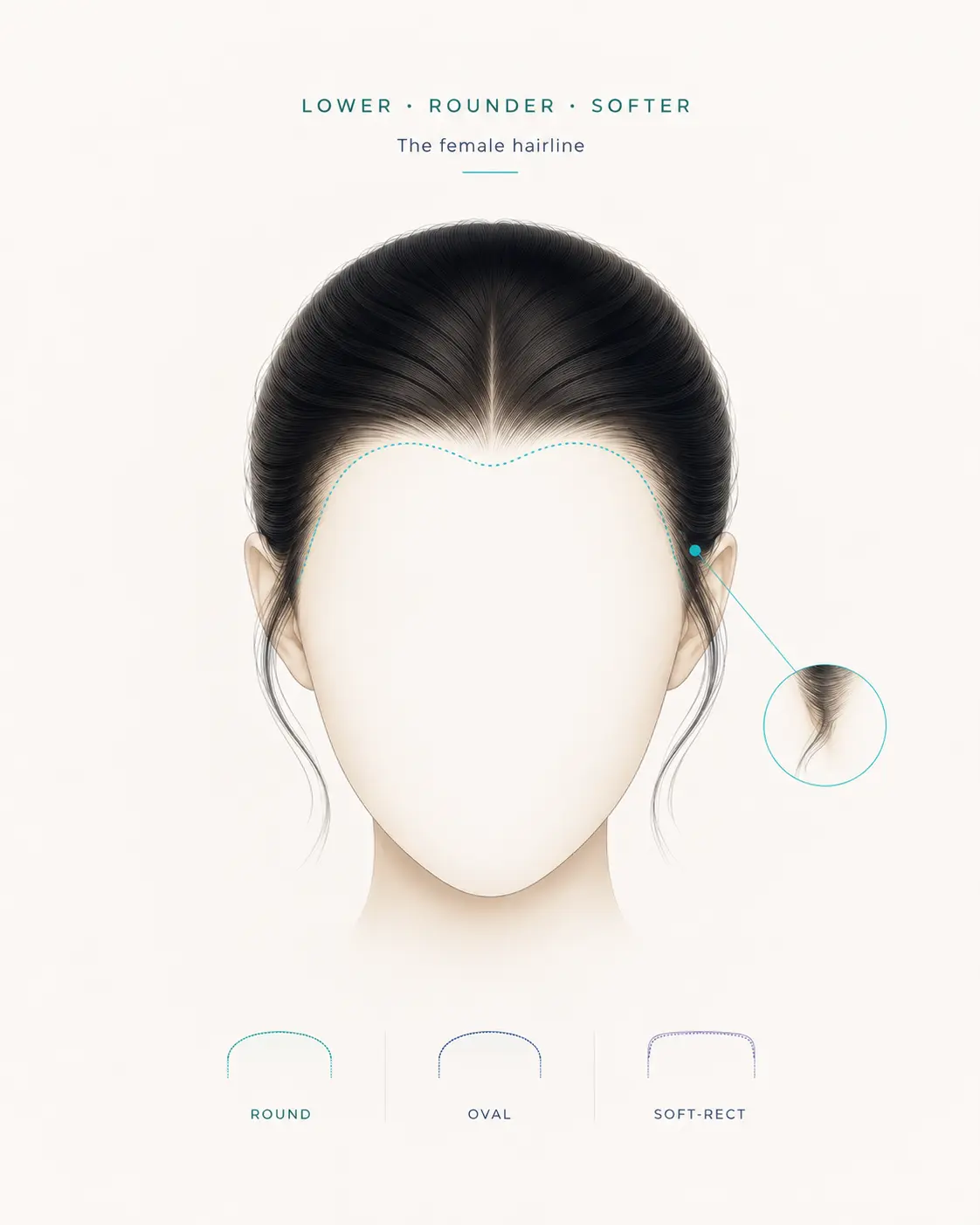
The female hairline frames the face — softness, balance, and expression. Its restoration is an exercise in artistry: recreating the micro-details, angulations, and natural irregularities that make it distinctly female.
A female hairline
is more than a boundary.
Unlike male hairlines, the female hairline sits lower, frames the face with softness, and carries micro-details that signal femininity. Restoring it requires as much artistry as surgery.
Lower Placement & Wider Arch
Female hairline placement depends on facial proportions, forehead height, and individual anatomy. In most cases, it sits lower and softer than a typical male hairline — but every plan is unique to the patient.
Micro-Irregularity & Natural Flow
The "micro" structure of a female hairline is never perfectly straight. The temple area requires careful direction planning so the result follows the patient's natural flow.
Temple Framing
For women who have lost temple hair through surgery (facelift, brow lift) or aging, precise graft placement restores the framing that defines a youthful, feminine appearance.
Scar Concealment
Hair transplantation may help camouflage suitable scars from previous facial procedures in the temple, sideburn, and post-auricular regions — especially when the scar tissue can safely support graft survival.
Understanding Your Case
Two different needs.
Two different plans.
Design-focused. Often stable.
For women born with a naturally high hairline or a large forehead. The donor area is typically stable, making surgical planning more predictable. The priority is design — shape, softness, and natural flow.
Medical-first. Stability-dependent.
For women experiencing progressive thinning across the top or crown. Medical stabilisation comes before any surgical discussion — and a combined approach is often more appropriate than surgery alone.
Understanding the Ludwig Scale
The Ludwig scale classifies female-pattern hair loss into three grades based on the degree of central thinning. Identifying your stage guides which treatments — medical, surgical, or combined — are most appropriate.
Ludwig Grade I
Earliest detectable stage. The frontal hairline remains intact while a slight widening of the central parting becomes visible.
- Central parting widens subtly when hair is combed
- More scalp shows under direct overhead light
- Ponytail volume slightly thinner than before
Medical therapy first. Minoxidil, hormonal evaluation, and nutritional review usually deliver meaningful improvement at this stage. At this point, surgery is rarely the responsible first step.
Ludwig Grade II
A clearly widened central part with diffuse thinning that begins to spread outward across the crown — the most common presentation we see in consultation.
- "Christmas tree" pattern visible from above
- Reduced density across crown and mid-scalp
- Styling no longer covers thinning areas reliably
Combined plan. Medical stabilisation first, then strategic transplantation to restore density where coverage matters most. Sequencing is critical.
Ludwig Grade III
Severe diffuse thinning across the entire crown. The scalp is clearly visible through remaining hair and styling no longer offers coverage.
- Significant scalp visibility under any lighting
- Crown density reduced beyond compensation by styling
- Donor stability must be confirmed carefully, as female donor zones may also show diffuse miniaturisation
Surgery may be considered when donor capacity is sufficient and the loss pattern is stable. In suitable cases, transplantation combined with ongoing medical therapy can improve visible density.
Diffuse Unpatterned
A distinct presentation where thinning extends into the donor zone itself — the sides and back of the scalp — making it the most complex pattern to plan for.
- Thinning visible across the entire scalp, not just crown
- Donor area shows reduced density on close inspection
- Often progresses more uniformly than patterned loss
Highly individualised. Donor capacity is the limiting factor. Surgery is only considered when long-term stability can be ensured — otherwise medical therapy alone is the responsible path.
Classification presented for educational purposes. A personal consultation is essential for accurate assessment.
Surgery is step two.
Understanding why
comes first.
Female hair loss is rarely a single-cause condition. Before any surgical discussion, our team conducts a thorough medical evaluation to rule out reversible causes — ensuring surgery is the right answer and timing is optimal.
Hormonal Profile Assessment
Androgens, oestrogen levels, and thyroid function are evaluated. Hormonal imbalances can drive hair loss independently of genetics — and are often treatable.
Nutritional Status
Serum ferritin, iron, zinc, and vitamin D are measured. Low ferritin may affect shedding, hair quality, and recovery potential, so it should be corrected before surgery when clinically relevant.
Loss Stability Assessment
Active, accelerating hair loss is a contraindication for surgery. Our specialists assess the rate and pattern of loss to confirm it has stabilised or can be stabilised before proceeding.
Dermatologic Scalp Evaluation
Inflammatory conditions (scarring alopecia, lichen planopilaris) must be identified and treated prior to surgery. A short course of topical steroids may be recommended.
Donor Area Evaluation
Unlike men, women's donor areas can be affected by diffuse thinning. Donor density and quality are carefully mapped to ensure sustainable graft availability before any plan is proposed.
Important: In women, the donor area is not always permanently stable. This is why donor mapping matters before any surgical plan is discussed.
Conditions we investigate before surgery
Both hypo- and hyperthyroidism can trigger diffuse hair loss. When clinically relevant, correcting thyroid imbalance may help reduce shedding and improve hair quality.
Low serum ferritin is one of the most common and overlooked causes of female hair loss. Correcting the deficiency can support recovery and improve the response to treatment.
Telogen effluvium following childbirth is temporary and typically resolves within 6–12 months. Surgery is not indicated during this phase.
Polycystic ovary syndrome elevates androgens, accelerating female-pattern hair loss. Medical management alongside surgery may improve long-term outcomes.
Certain medications — including some contraceptives, antidepressants, and blood thinners — can cause or exacerbate hair thinning and must be flagged during evaluation.
A plan built around your hair,
not a protocol.
Female hair restoration is rarely one-size-fits-all. Our core team combines medical and surgical options into a personalised strategy — sometimes phased, always evidence-based.
One of the most evidence-supported non-surgical options for women. May thicken existing hair shafts, help slow progression, and support scalp stabilisation in suitable patients. Pre-operative use may also be recommended to help stabilise shedding before surgery.
When scalp inflammation is present, a short course of topical anti-inflammatory treatment may be considered under medical supervision. Not a standalone solution — always assessed case by case.
PRP uses growth factors from your own blood to support the scalp environment and may improve hair quality in selected patients. A natural adjunct to both medical and surgical treatment.
Regenera Activa® may be considered as a supportive, non-surgical option in selected early-stage thinning cases. It is not a replacement for medical diagnosis, long-term stabilisation, or surgery when surgery is truly indicated.
Iron, ferritin, zinc, biotin, and vitamin D — when deficient, targeted supplementation can yield meaningful improvement in hair density before any other intervention.
For most women, our team designs a multi-modal approach: medical stabilisation first, then surgical restoration, then ongoing maintenance. Each element reinforces the next.
- No-shave or minimal-shave FUE available for women
- Donor harvested from the nape and sides — areas less affected by female-pattern loss
- Natural hairline design using single-hair grafts at the front
- Return to styling in 7–10 days
- Full results visible at 12–18 months
For selected patients, no-shave or partial-shave FUE may be possible. Suitability depends on donor density, graft number required, hairstyle, and the area being restored. This is assessed individually — not offered as a blanket option.
- Comprehensive donor mapping before any commitment
- Strategic recipient design maximises visual impact per graft
- Medical therapy used to protect remaining donor hair
- Staged approach available when donor supply is limited
Not all women are surgical candidates. An honest evaluation may conclude that medical therapy alone — or a staged approach — will deliver better long-term results than immediate surgery.
The most underused tool in female hair restoration.
Minoxidil has strong clinical support — but its value depends on correct indication, consistency, and realistic expectations. Many women stop too early, miss the stabilisation window before surgery, or underestimate what it can do when paired with the right protocol. Our team provides clear, evidence-based guidance so patients get the most from every option before and after surgery.
Premature discontinuation is the most common mistake. The follicular cycle takes months to respond — patience is essential to accurate assessment.
Temporary increased shedding can occur during the first weeks as follicles transition through the growth cycle. It is a known response and usually settles with continued use.
In suitable patients, pre-operative use helps stabilise the scalp before surgery. Post-operatively, continued use supports the long-term environment for transplanted and existing hair.
Who is the right candidate?
Female hair transplantation can be effective for a range of carefully selected patients. The key is a thorough, honest assessment — not every woman needs surgery, and not every woman who wants it is yet ready for it.
Women with High Hairlines
Born with a naturally high or large forehead, feeling that hairline proportions are off. Hair transplantation can lower and reshape the hairline to better frame the face — often transformative with relatively few grafts.
Female-Pattern Hair Loss
Stable thinning across the crown with adequate donor density. Surgery can restore meaningful density — particularly when medical therapy has plateaued or the visual impact on daily life is significant.
Aging & Receding Hairlines
Gradual retreat of the temples and frontal hairline with age. Hair transplant subtly restores a youthful framing without dramatic change — often combined with PRP to support remaining native hair.
Transgender Women (MTF)
Achieving a feminine hairline is one of the most meaningful aspects of gender affirmation. Dr. Demir designs hairlines that complement the facial structure with sensitivity, precision, and a strong understanding of feminine hairline aesthetics.
Five factors that shape your plan.
Every consultation with Dr. Demir follows the same framework — not a script, but a discipline. Each factor informs the next until the most effective, honest treatment plan takes shape.
Loss Stability
Is the loss stable, slowing, or accelerating? Timing surgical intervention correctly is critical.
Donor Quality
Density, calibre, and extent of thinning in the donor zone — the foundation of any surgical plan.
Medical Status
Hormonal, nutritional, and dermatologic factors that must be addressed before or alongside surgery.
Hair Characteristics
Calibre, curl, colour contrast with the scalp — these determine visual density impact per graft.
Goals & Expectations
Alignment between what surgery can achieve and what the patient expects is essential for satisfaction.
Your hair has a story
worth protecting.
Whether you're dealing with a high hairline, diffuse thinning, or decades of gradual loss — the right plan starts with an honest conversation. One patient. One core team. One standard.